Recent public debates about Medicaid have increasingly centered on “waste, fraud, and abuse,” often treating the concept as both a diagnosis and a solution. Yet recent polling suggests a more complicated reality.
A March 2026 Hart Research poll found that while voters express concern about fraud in basic needs programs, they continue to hold overwhelmingly favorable views of Medicaid across the political spectrum, and most prioritize ensuring access to care over preventing misuse. This tension between concern about fraud and support for the program itself helps explain the persistence of the current policy debate.
Balancing fraud detection policies with the need for services
Fraud matters to the public. But it is not the primary lens through which they view Medicaid. When forced to choose, voters consistently place greater weight on whether programs reach those in need than on whether every dollar is perfectly controlled. At the same time, claims of widespread fraud remain politically salient, shaping how policymakers frame proposals to reform or reduce Medicaid spending. Some go so far as to use them to justify the nearly $1 trillion in Medicaid cuts contained in HR 1.
Program integrity is no longer confined to enforcement after the fact.
This dynamic is increasingly visible in federal and state policy. Executive Order 14395 issued March 16, 2026, established a federal government-wide task force to coordinate fraud detection and program integrity efforts across federal benefit programs, including Medicaid. The initiative reflects a broader shift. Program integrity is no longer confined to enforcement after the fact but is being embedded into the structure of eligibility and payment itself.
At the same time, recent federal actions highlight the challenges of correctly identifying fraud. In early 2026, federal officials publicly raised concerns about widespread fraud in New York’s Medicaid program based on claims data analysis. The administration later acknowledged a significant error in those findings, underscoring how easily anomalies in complex datasets can be misinterpreted as evidence of fraud. As federal and state agencies increasingly rely on data-driven methods to detect improper payments, the distinction between statistical outliers and intentional misconduct can become blurred.
Defining “high-risk”
The Centers for Medicare & Medicaid Services (CMS) sent a letter late last month to state Medicaid directors directing states to undertake accelerated revalidation of Medicaid providers, particularly those categorized as “high-risk,” and to submit comprehensive two-year provider revalidation strategies focused on enrollment oversight, data accuracy, and coordination with law enforcement. CMS requested that states notify the agency within 10 days of their plans to conduct swift revalidation of high-risk providers and submit full strategies within 30 days.
While ensuring that enrolled providers are legitimate is a reasonable objective, the practical meaning of “high-risk” remains only partially defined at the federal level. CMS is also encouraging states to conduct off-cycle or more frequent revalidation beyond the traditional five-year cycle and to prioritize providers who have not recently been screened. In practice, this could create a significant new administrative burden for states and providers alike, especially if broad provider categories are swept into enhanced screening and documentation requirements.
Early state experiences offer some perspective. In Minnesota, services flagged for heightened scrutiny have included home- and community-based supports, behavioral health services, and other labor-intensive care delivered outside traditional clinical settings. CMS identifies these types of services as high-risk in part because they are more difficult to monitor and verify, relying heavily on documentation rather than direct observation. At the same time, these are also areas where care delivery is inherently variable and decentralized, raising the possibility that “risk” reflects administrative complexity as much as demonstrated patterns of fraud.
Defining waste, fraud, and abuse
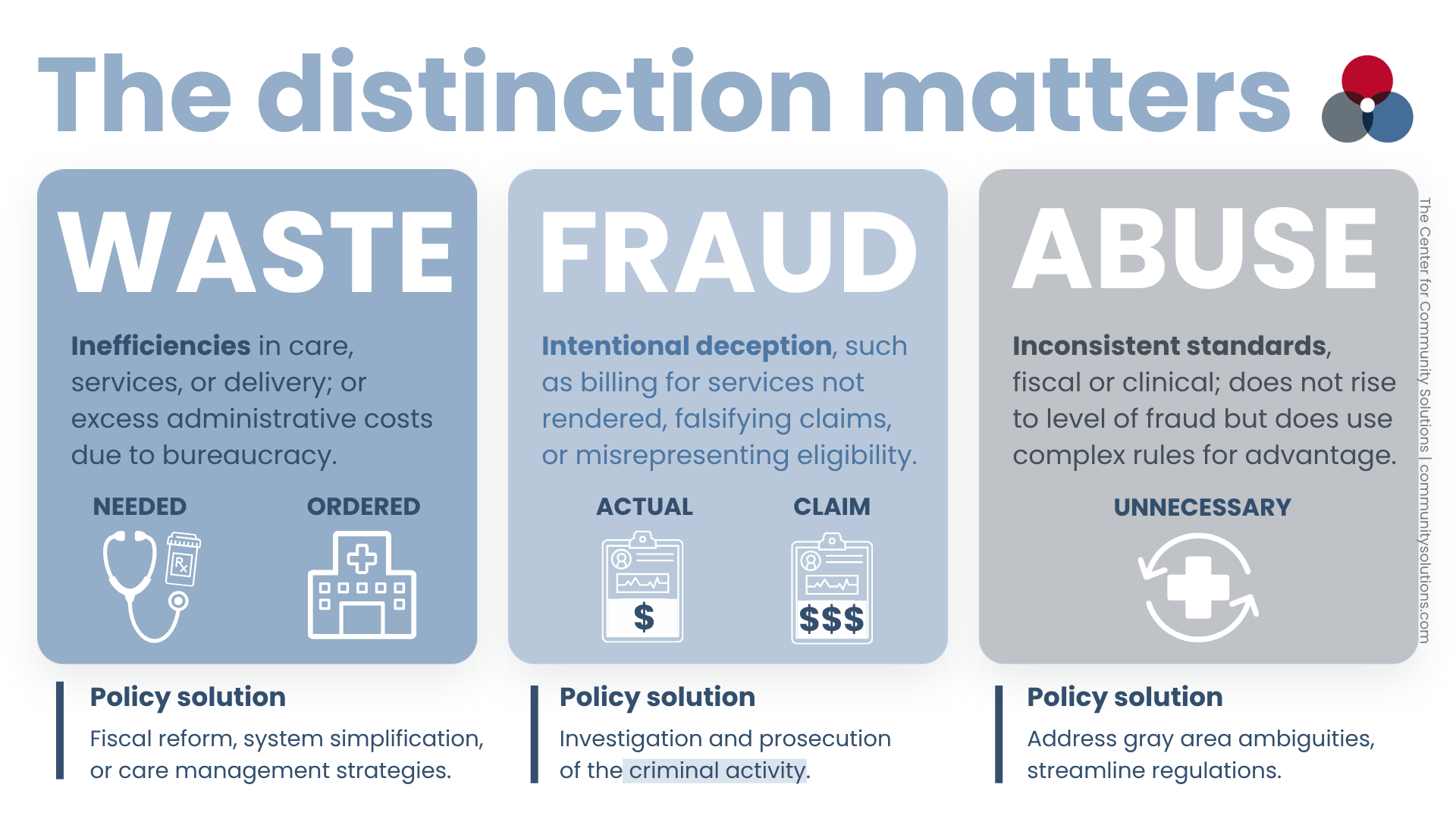
“Waste, fraud, and abuse” is often invoked as a single, unified concept, but the distinctions matter.
- Waste generally refers to inefficiencies in care delivery, including unnecessary services or avoidable utilization.
- Fraud involves intentional deception, such as billing for services not rendered, falsifying claims, or misrepresenting eligibility.
- Abuse occupies a gray area between the two, encompassing practices that may be inconsistent with sound fiscal or clinical standards but do not rise to the level of fraud.
The policy tools required to address each differ significantly.
- Waste may require payment reform or care management strategies.
- Fraud calls for investigation and prosecution.
- Abuse often reflects ambiguities in clinical or billing standards,
Yet in practice, these categories are frequently collapsed, allowing measures of “improper payments” to stand in for fraud, even when they reflect administrative or technical issues rather than intentional wrongdoing.
Medicaid fraud is not new, but it is growing more sophisticated
Concerns about Medicaid fraud are not new. Since the program’s early years, policymakers have grappled with how to detect and prevent improper payments in a system that serves millions of beneficiaries and relies on a diverse network of providers.
What has changed over time is less the existence of fraud than the tools used to identify it. Advances in data analytics, expanded service delivery models, and increasing administrative complexity have all influenced how fraud is measured and perceived.
Recent work by the Government Accountability Office highlights how fraud is also becoming more sophisticated. Increasingly, fraud schemes are not limited to individual bad actors but involve organized efforts that exploit the structure of benefit programs at scale. As federal and state agencies strengthen controls—through verification, data analytics, and pre-payment review—those seeking to defraud the system adapt in response, identifying gaps in eligibility systems, documentation processes, and oversight mechanisms. This underscores the challenge of maintaining effective oversight in a system where both detection tools and fraudulent schemes continue to evolve.
How Ohio prevents and detects Medicaid fraud
Recent testimony before Ohio’s House and Senate Medicaid Committees illustrates the extent to which Ohio already operates a robust program integrity system. Scott Partika, Director of the Ohio Department of Medicaid, described a multi-layered approach that includes provider screening, eligibility verification, data analytics, and coordinated investigations with managed care plans and law enforcement. Tools such as Electronic Visit Verification, prior authorization, and third-party liability enforcement are designed to ensure services are delivered and appropriately billed.
Ohio Attorney General Dave Yost emphasized an active enforcement role, with a nationally recognized Medicaid Fraud Control Unit responsible for investigating and prosecuting provider fraud, increasingly supported by data mining and artificial intelligence. At the same time, Tiffany Ridenbaugh, Chief Deputy Auditor of the Ohio Auditor’s Office, highlighted ongoing oversight through financial audits, compliance reviews, and targeted program evaluations, identifying both improper payments and administrative weaknesses, particularly in eligibility systems and documentation.
Ohio’s Medicaid fraud detection protocol examines both individual and system issues.
- Eligibility screening, analytics, and services billing
- Data mining to support investigation and prosecution
- Financial audits and compliance reviews
Together, these perspectives highlight an important distinction. Enforcement activity focuses on prosecutable fraud, while audit findings often reflect administrative and system-level challenges. These are two fundamentally different issues that are frequently combined in broader policy discussions.
A significant share of improper payments arises not from fraud, but from administrative and documentation errors.
Fraud, error, and the structure of the system
At the level of individual cases, fraud is real and prosecutable. Ohio’s Medicaid Fraud Control Unit regularly brings cases involving billing for services not rendered, falsified timesheets, and identity-based schemes. These cases are concrete and visible, and they play an important role in maintaining program accountability.
But broader program reviews tell a different story. A significant share of improper payments arises not from fraud, but from administrative and documentation errors, particularly in eligibility verification, renewals, and billing compliance. These are fundamentally different from intentional misconduct.
This distinction matters because policy responses often do not differentiate between error and intent. As policymakers respond by adding layers of verification, documentation, and pre-payment controls, they may be addressing symptoms of administrative complexity rather than fraud itself.
There is also a structural dynamic at work. Each new requirement, whether a documentation standard, verification step, or prior authorization rule, creates additional opportunities for technical noncompliance. Missed documentation, timing discrepancies, or eligibility mismatches can be captured in data systems as improper payments. Over time, this can create a feedback loop. Increased complexity generates more findings, which are interpreted as evidence of risk, prompting further controls.
In this way, a system designed to detect fraud can begin to measure its own complexity, capturing administrative irregularities as evidence of risk even when they do not reflect intentional misconduct.
A note on incentives and definitions
When I think about how these dynamics play out in practice, I am reminded of my time as Ohio’s Medicaid director, when I attempted to implement a policy to competitively bid adult diapers in order to save $20 million. One of the most conservative members of the legislature opposed the change, not on policy grounds, but because one of the largest durable medical equipment providers in his district relied on that revenue. What counted as “waste” often depended on who benefited from the existing arrangement.
The same dynamic applies, in different ways, to fraud. Definitions are not purely technical. They are shaped by policy choices, administrative structures, and political incentives.
What is counted as improper or fraudulent often reflects how the system is designed to measure it.
Public perception and policy choices
Public opinion research suggests that voters recognize both sides of this tension. While large majorities express concern about fraud in basic needs programs, they also overwhelmingly view programs like Medicaid as a good investment and believe they primarily help people who need support. Importantly, when asked to prioritize, voters are more likely to emphasize ensuring access to assistance than preventing fraud.
This has direct implications for policy. Claims of widespread fraud may be politically salient, but they do not automatically translate into support for funding reductions. In fact, proposals to freeze or cut funding in response to fraud concerns tend to be viewed skeptically, particularly when they are seen as harming vulnerable populations.
Recent analysis of federal actions reinforces this point. In Minnesota, federal officials cited fraud concerns in pausing Medicaid funding to the state and subsequently used the episode to support broader initiatives, including nationwide provider revalidation and expanded scrutiny of “high-risk” services.
While addressing fraud is a legitimate objective, the use of a single state’s experience to justify system-wide policy changes highlights how fraud can function not only as a program integrity issue, but as a rationale for increased federal intervention and administrative control.
What about lived experience?
One notable absence in these discussions is the perspective of Medicaid beneficiaries themselves. The debate is largely shaped by those who see the issue through the lens of oversight and accountability. Missing is the experience of those who rely on Medicaid for their care, individuals for whom eligibility processes, documentation requirements, and provider participation are not abstractions but daily realities.
Policies designed to strengthen program integrity are often evaluated based on their ability to detect improper payments, but less attention is paid to how they affect access to care, continuity of coverage, and the practical ability of beneficiaries to navigate the system.
Administrative complexity accounts for a substantial share of improper payments, but intentional fraud and systemic waste are still real. Every dollar lost to fraudulent billing, falsified claims, or ineligible enrollments is a dollar no longer available for the children, seniors, and individuals with disabilities who rely on Medicaid for essential care.
Program integrity, properly understood, is not the same as restricting access. When enforcement targets prosecutable fraud through data analytics and coordinated investigation, as Ohio has demonstrated, it frees up resources, deters bad actors, and sustains public confidence in the program.
Conclusion
Program integrity should remain a central component of Medicaid. But clarity about what is being measured, and what is driving those measurements, is essential. As oversight mechanisms expand, policymakers face a familiar tradeoff. A system that is too permissive invites abuse. But a system that is too complex may generate its own version of it, producing findings that reflect administrative burden rather than misconduct.
What remains largely absent from this debate is the voice of Medicaid beneficiaries, even as policy choices about fraud and oversight continue to shape their access to care. When those perspectives are missing, policies designed to strengthen program integrity may do so at the expense of the very people the program is intended to serve.